Facial Reanimation Surgery
What is Facial Reanimation Surgery?
Facial reanimation surgery is a specialized surgical approach designed to restore facial movement and symmetry in individuals with facial paralysis. This paralysis can result from various causes, including facial nerve damage due to trauma, tumors, Bell’s palsy, or other neurological conditions. The goal of facial reanimation surgery is to improve both the functional and aesthetic aspects of facial expressions.
Several surgical techniques may be employed in facial reanimation surgery, depending on the underlying cause and extent of facial nerve damage.
As the time from facial nerve injury increases, atrophy and scarring will occur in the facial muscles. Unlike the treatment options for acute facial nerve paralysis which are almost always aimed at reinnervating functional facial muscles, the treatment options for chronic facial nerve paralysis (greater than 1 year) can be separated into two broad categories of reversible and irreversible injuries.
In cases where it is unknown whether the patient has reversible or irreversible facial nerve injury, history, physical exam and diagnostic electrophysiologic testing are essential.
Patients with functional facial muscles have reversible injuries, and treatment is aimed at reinnervation of these muscles through repair of the facial nerve or transferring another nerve to power the branches of the the facial nerve close to the muscles of the face.
Patients whose facial muscles are no longer functional have irreversible injuries and typically require muscle transfers or static slings to restore facial form and function.
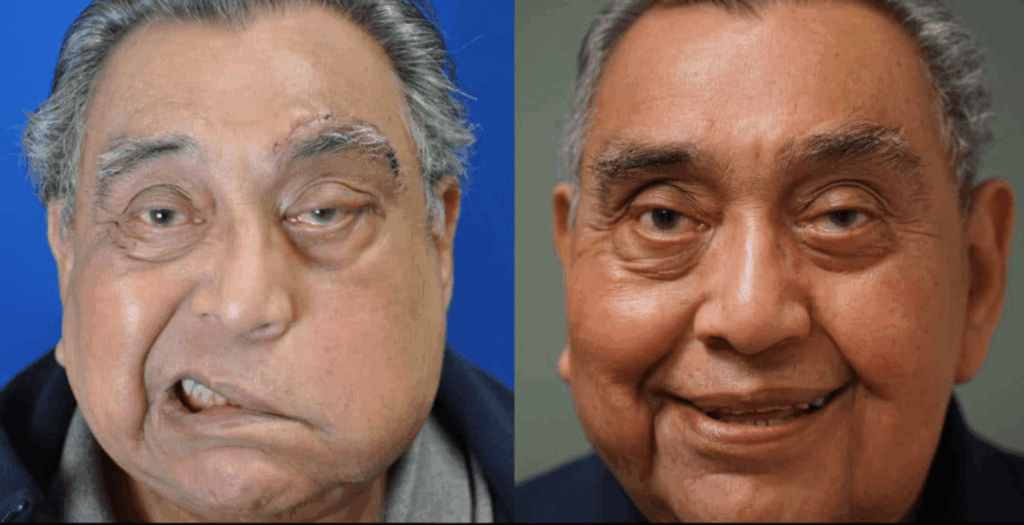
Photo Gallery | Before & After Facial Reanimation



Types of Facial Reanimation Surgery
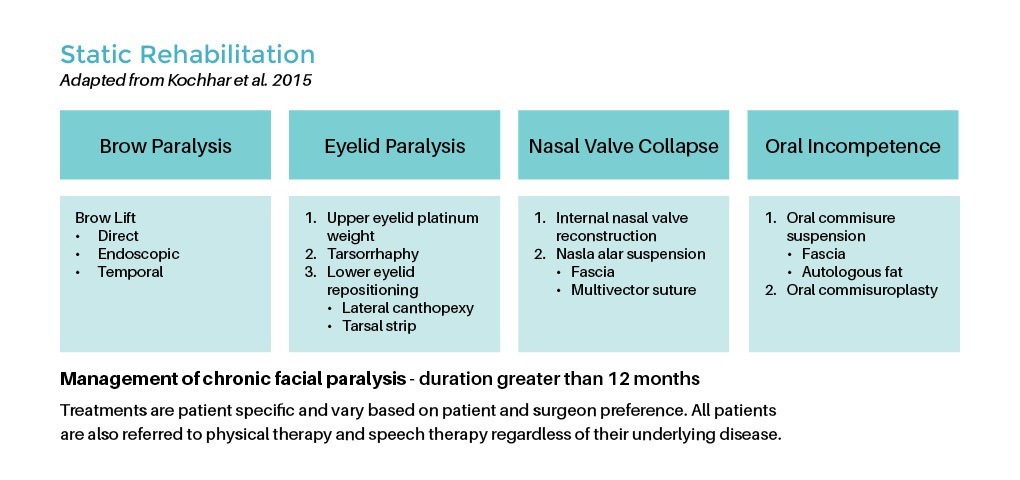
Static Procedures
Static procedures do not lead to active purposeful movement. However, static facial reanimation plays an essential role in the treatment of facial paralysis and should not be overlooked. Static facial reanimation relies heavily on elevation and positioning of several key areas on the face and is often performed in combination with dynamic procedures, or those that do lead to purposeful movement.
Static suspension is often performed on the following areas:
- Elevating the droopy eyebrow to prevent visual field obstruction and to create symmetry with the opposite side
- Elevating the nasal ala and midface to improve breathing and repair collapse of the external nasal valve which is affected by facial paralysis
- Elevating the droopy oral commissure of the affected side to provide immediate restoration of symmetry. Elevation of the oral commissure not only provides symmetry but can also make it easier to speak, eat and drink on the affected side. This can be done in combination with nerve reinnervation or muscle transfer to correct asymmetry while waiting for the new nerves and muscles to activate.
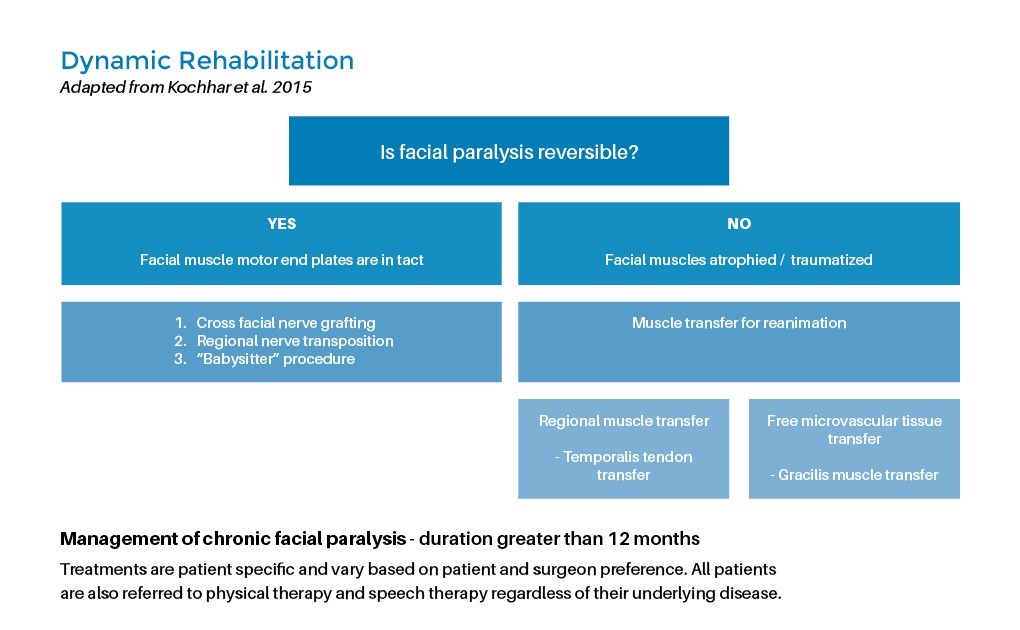
Dynamic rehabilitation
Dynamic rehabilitation is required to restore facial tone, symmetry and purposeful synchronized facial movements.
Various options exist for dynamic facial nerve reanimation that includes:
- Nerve grafting
- Crossover techniques
- Nerve transfer or transposition
- Local muscle/tendon transfer
- Free muscle transfer
Facial Reanimation Surgery Specialist


Written and reviewed by:
The Pacific Neuroscience medical and editorial team
We are a highly specialized team of medical professionals with extensive neurological and cranial disorder knowledge, expertise and writing experience.
Last Updated: