Deep Brain Stimulation for Parkinson’s Disease
What is Deep Brain Stimulation For Parkinson’s Disease?
“On-Off” Time in Parkinson’s Disease (PD)
Unfortunately, at some point along the course of the diagnosis of Parkinson’s disease (PD), the brain no longer responds consistently to the medications. The effective window (known as ON time) is shorter, and thus there is more OFF time (when the patient feels slow, sluggish, or frozen because the medications haven’t kicked in yet or have worn off too soon).
Motor Complications in Parkinson’s Disease
In addition, there are increased dyskinesias (involuntary movements), which refer to abnormal involuntary movements (not including tremor). ON/OFF fluctuations and dyskinesias are known collectively as motor complications.
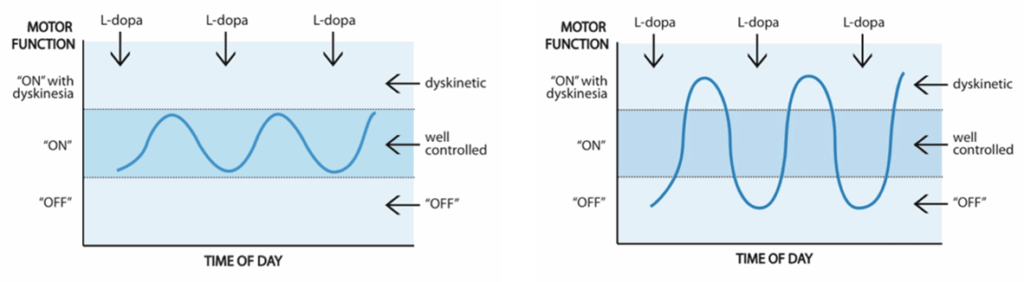
Whereas levodopa concentration fluctuations can contribute to unpredictable shifts between ON and OFF time, Deep Brain Stimulation remains constant through the day, meaning that there is consistent efficacy throughout the day.
Deep Brain Stimulation for Parkinson’s Disease Treatment
Patients note a significant improvement in ON time – meaning an addition of 5 good hours of productivity during the day. Deep Brain Stimulation (DBS) helps free patients from the worry of whether their medication is going to kick in at the right time for them to drive to work, participate in a meeting, have a meal, or pay a visit to a friend. This improves quality of life dramatically.
For many patients with Parkinson’s disease who continue to experience challenging symptoms, a state-of-the-art technology introduced in 2020 at Pacific Neuroscience Institute can provide comfort and relief.
The DBS surgically-implanted device called Percept™ PC Neurostimulator with BrainSense™ technology detects patient-specific brain signals and provides feedback to optimize therapy for patients with Parkinson’s disease. Benefits include improvements in tremors, rigidity, slowness of movement and overall quality of life.
Our movement disorders neurology and restorative neurosurgery specialists provide DBS expertise and experience. The first in Providence health system to use Percept™ PC with BrainSense™, this breakthrough in monitoring and treatment technology can be considered for patients who need to take their current medications too frequently, or who can no longer tolerate their current treatment regimen. This DBS system is available for new patients as well as for updating older implanted DBS systems.
Patients receive a comprehensive and personalized medical and treatment assessment to determine of DBS is an appropriate choice.
Deep Brain Stimulation For Parkinson’s Disease Specialist

Written and reviewed by:
The Pacific Neuroscience medical and editorial team
We are a highly specialized team of medical professionals with extensive neurological and cranial disorder knowledge, expertise and writing experience.
Last Updated: